Stress incontinence is characterized by involuntary passage of urine following strain on the pelvic floor such as coughing, straining at stools or even minor changes in posture. The leak of urine is painless and sudden and varies from a few drops to a gush of urine depending on the severity of damage.
Although stress urinary incontinence is a very common problem (some studies estimate the prevalence in the range of 50% in older women), the majority of women do not seek treatment out of shame and taboos regarding discussing these problems.
The confirmation stress urinary incontinence is by a simple test called urodynamic sstudy which is done in many centres in India. This virtually confirms the diagnosis while ruling out other forms of incontinence.
While very mild stress urinary incontinence may be managed by exercises of the pelvic floor muscles or by use of pessary (especially during pregnancy), the mainstay of treatment is surgery.
The older treatments of stress incontinence involved a lot of dissection of the pelvic floor and were morbid procedures. However, the surgical treatment of stress incontinence has been revolutionized in the past few decades by the advent of procedures involving the use of a vaginal tape.
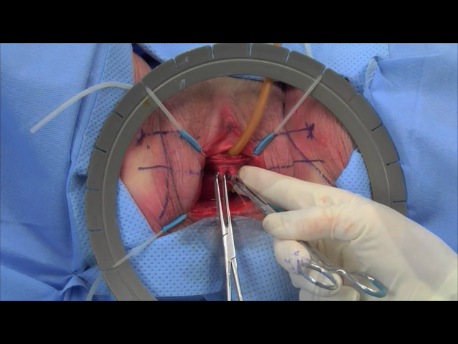
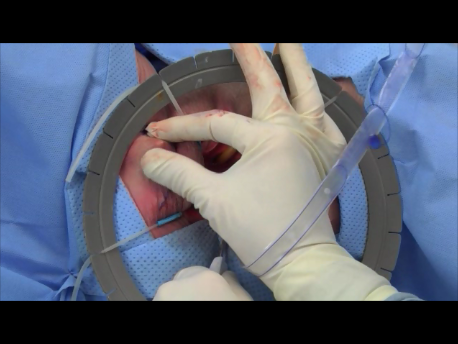
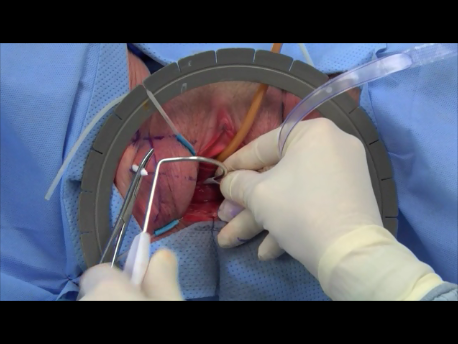
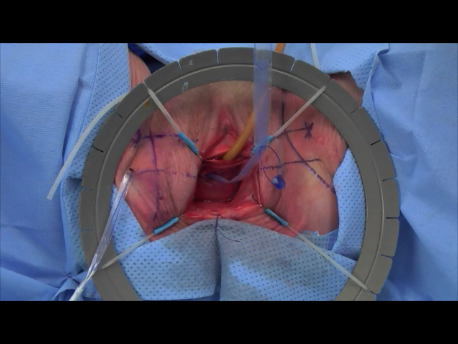
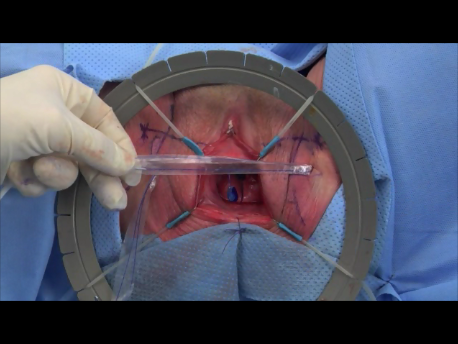
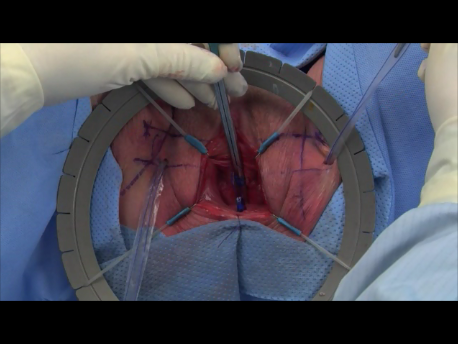
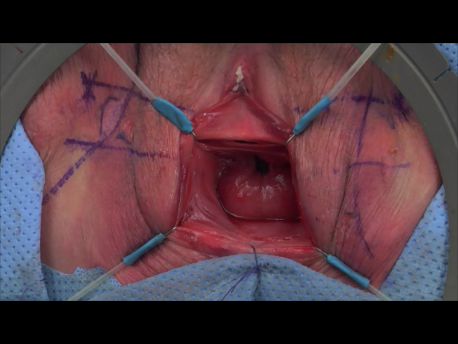
The tension free vaginal tape uses a non-absorbable tape made of prolene. This tape is passed around the urethra via a vaginal incision. It is brought out at the skin just above the pubis (the tension free vaginal tape or TVT procedure) or just lateral to the labia near the medial aspect of the thigh (the TVT-O procedure). The TVT-O procedure ias a simpler procedure with virtually no risk of bladder injury and low risk of hemorrhage. The success rates of the two procedures are about 95%.
In rare cases of failure or in women requiring an abdominal surgery, the procedure of choice is the Burch colposuspension. This can be done by laparoscopy. The tissue behind the urethra and on the sides of the vagina is fixed to a ligament over the pubic pone (iliopectineal ligament) with non-absorbable sutures.
This is especially useful for women with prolapse or laxity of the anterior aspect of the vagina (cystosele).
Rarely, in women with multiple surgical failures (4 or more) or with congential defects of the pelvic floor, an artificial urinary sphincter or urethral closure may be necessary.