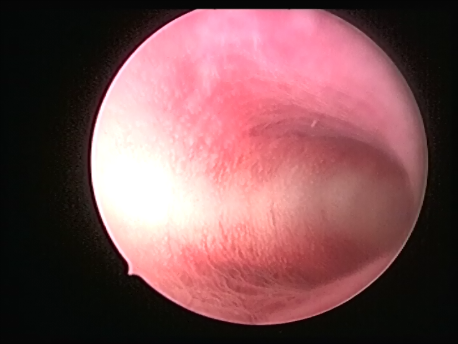
Hysteroscopy means peeping inside the uterine cavity with the help of a fine telescope varying between 2-4mm in diameter. Today a large number of surgeries can be performed via hysteroscopy due to advances in technology and instrumentation. These procedures do not involve any cut on the body and, hence, are virtually painless. The patient can be admitted on the day of the surgery and, if a laparoscopy is not needed, discharged in a few hours.
Hysteroscopy can be performed for the following indications :
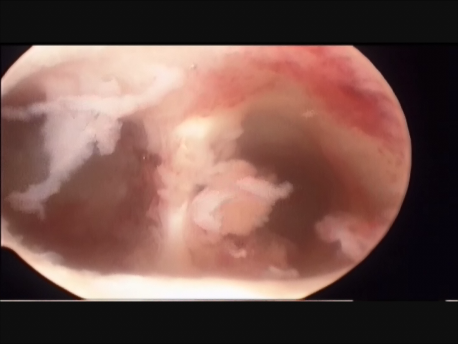
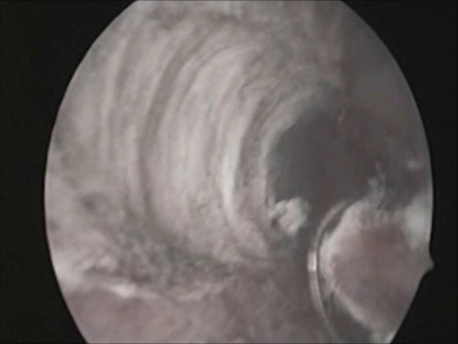
- Infertility and recurrent loss (Subfertility): Infertility means the inability to conceive and recurrent pregnancy loss means loss of 3 or more (in practice, usually 2 or more) consecutive early pregnancy (less than 5 months). Uterine pathology such as abnormal shape (septum or the T shaped uterus), submucous fibroids or polyps, and intrauterine adhesions can cause subfertility. Tubal block due to spasm or mucus plugs can contribute to infertility and can be opened by hysteroscopic cannulation.
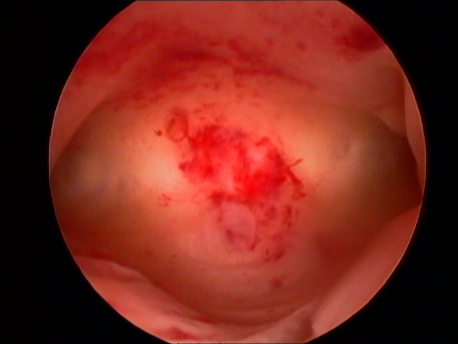
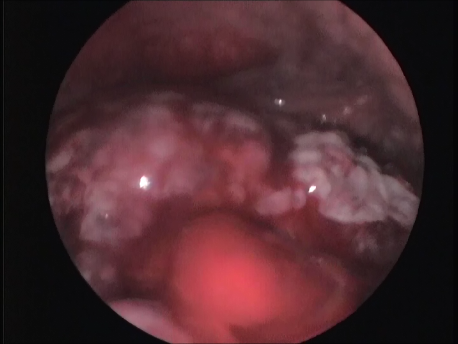
- Abnormal uterine bleeding: Heavy, prolonged or irregular bleeding can be caused by submucous fibroids and polyps.
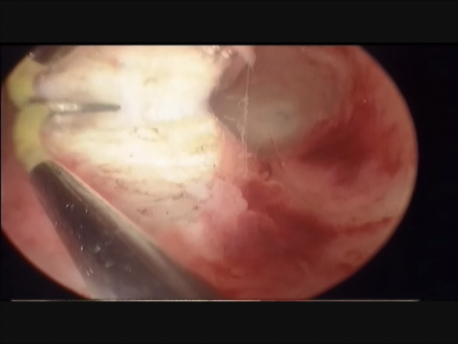
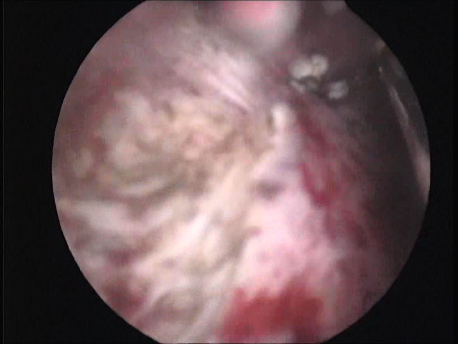
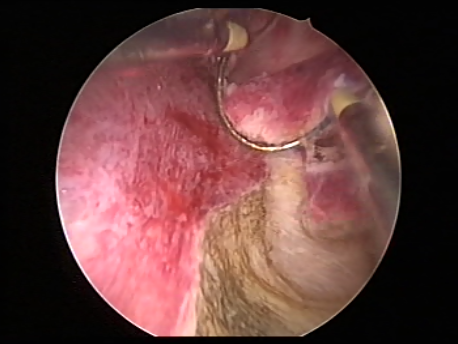
- Intrauterine foreign bodies: Missing copper T embedded in the uterine wall or retained fetal bones or pregnancy following a miscarriage can contribute to irregular bleeding, infection or subfertility.